Coronary Calcium Score: What It Means and Why It Matters
A clear, patient-friendly guide to the coronary artery calcium (CAC) score: what it measures, what the numbers mean, who should consider the test, and how it guides heart-disease prevention under the 2026 ACC/AHA dyslipidemia guideline.


Heart disease often develops quietly. Many people feel completely fine for years while cholesterol plaque slowly builds inside the arteries that supply the heart. A coronary artery calcium score, also called a CAC score or simply a calcium score, is one tool that can help detect hidden plaque before symptoms begin.
This test is not for everyone, and it does not replace a thoughtful visit with your clinician. But for the right patient, it can be a powerful way to personalize heart disease prevention.
The 2026 ACC/AHA/Multisociety Dyslipidemia Guideline emphasizes earlier prevention, healthy lifestyle habits, selective use of coronary calcium scoring, and more personalized LDL cholesterol goals based on each person's risk.
1. What is a coronary calcium score?
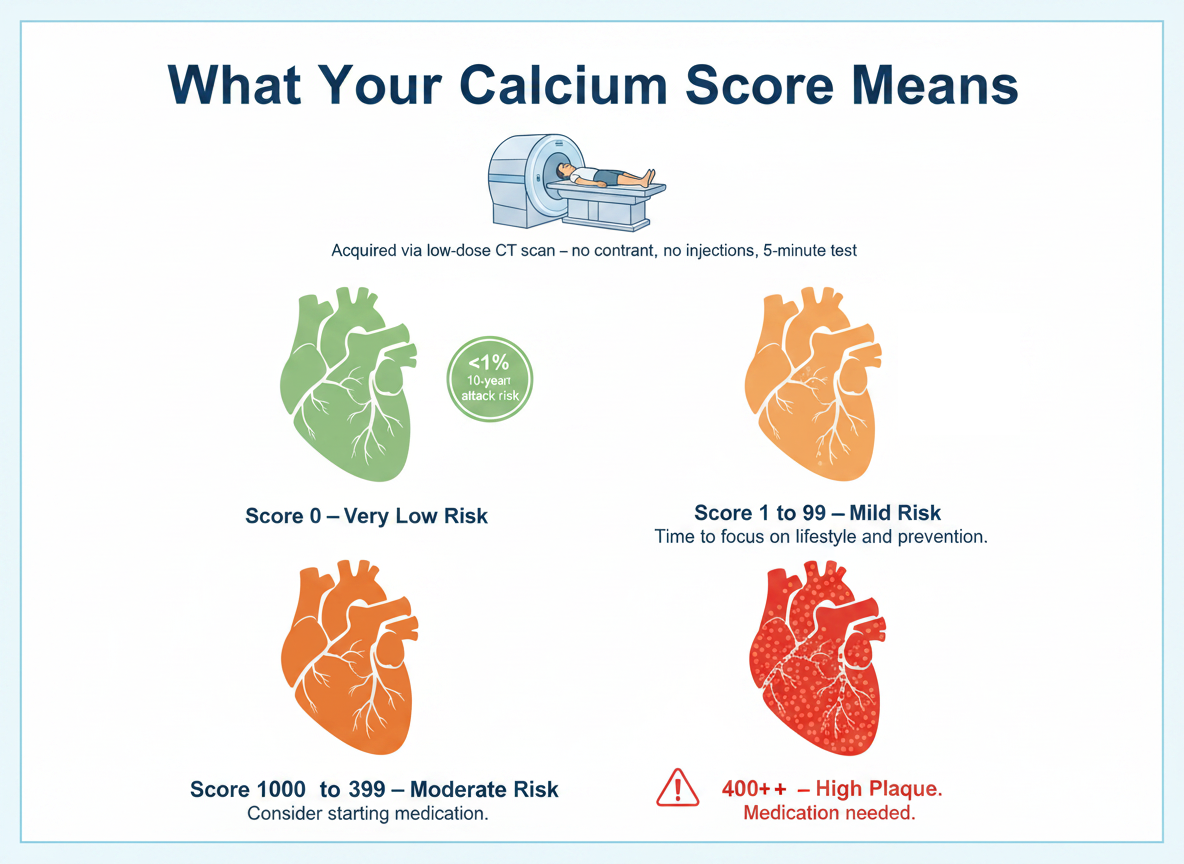
A coronary calcium score is a special CT scan of the heart. It looks for calcium deposits in the coronary arteries, which are the blood vessels that bring oxygen-rich blood to the heart muscle.
Calcium in these arteries is a sign of atherosclerosis, also known as plaque buildup. The scan usually does not require IV dye or needles, and the test often takes only a few minutes.
The result is reported as a number called an Agatston score. It is also more commonly referred to as the CAC (Coronary artery Calcium) score. A higher score usually means there is more calcified plaque in the heart arteries.
2. Why does calcium in the arteries matter?
Calcium in the coronary arteries is not the same as calcium in your bones. It also does not mean you ate too much calcium.
Coronary calcium usually means that cholesterol plaque has been present long enough for the body to form calcium within it. In simple terms, calcium is a marker that plaque exists.
A calcium score helps answer an important question: "Do I already have evidence of coronary artery disease, even if I feel fine?"
The 2026 ACC/AHA/Multisociety Dyslipidemia Guideline supports selective use of CAC scanning when there is uncertainty about a person's true risk and when the result would help guide cholesterol-lowering treatment.
3. What do the calcium score numbers mean?
Most calcium score reports use these general categories:
- 0 — No visible calcified plaque. Lower short-term risk.
- 1–99 — Mild calcified plaque. Risk is higher than zero.
- 100–299 — Moderate plaque burden. Cholesterol-lowering treatment is usually recommended.
- 300–999 — High plaque burden. More aggressive prevention is usually needed.
- 1000 or higher — Very high plaque burden. This often requires very aggressive cholesterol lowering.
The 2026 guideline brings back LDL cholesterol treatment goals. For people with CAC 1–99, an LDL-C goal of <100 mg/dL is recommended. For CAC 100–299, an LDL-C goal of <70 mg/dL is recommended. For CAC ≥1000, an LDL-C goal of <55 mg/dL is recommended.
In plain English: the higher the calcium score, the lower we usually want the LDL cholesterol to be.
4. Who should consider getting a calcium score?
A calcium score is most useful when you and your clinician are unsure how aggressive your prevention plan should be.
The 2026 ACC/AHA/Multisociety Dyslipidemia Guideline recommends selective CAC testing for men older than 40 and women older than 45 who have borderline or intermediate 10-year risk and where knowing the CAC score would help decide whether to start a statin or other LDL-lowering therapy.
A CAC score may be helpful if you have risk factors such as:
- Borderline or moderately high cholesterol
- High blood pressure
- Family history of early heart disease
- Past or current smoking
- Diabetes risk or prediabetes
- Chronic kidney disease
- Inflammatory conditions such as rheumatoid arthritis or lupus
- Early menopause
- Pregnancy-related risk factors, such as preeclampsia or gestational diabetes
- Higher-risk ancestry, including South Asian or Filipino ancestry
- Uncertainty about starting a statin
The updated guideline recommends using the PREVENT-ASCVD risk calculator instead of the older Pooled Cohort Equations for primary prevention adults ages 30–79. PREVENT estimates both 10-year and 30-year risk and helps guide cholesterol-lowering decisions.
5. Who usually does not need a calcium score?
A calcium score is usually not needed if the result will not change the plan.
For example, you may not need a CAC test if:
- You already have known coronary artery disease, a prior heart attack, a stent, or bypass surgery.
- Your LDL cholesterol is 190 mg/dL or higher, where cholesterol-lowering treatment is usually already recommended.
- You have symptoms that could suggest a blocked artery, such as chest pressure with activity. In that case, you may need a different type of heart test.
- You are already committed to aggressive prevention and the result would not change your treatment.
- You are very low risk and the result is unlikely to change management.
The key idea is simple: do the test when the result can change the decision.
6. What is the PREVENT risk calculator, and why does it matter?
The PREVENT-ASCVD calculator is a newer heart risk calculator recommended in the 2026 ACC/AHA/Multisociety Dyslipidemia Guideline. It is used for adults ages 30–79 who do not already have known cardiovascular disease. It estimates a person's risk of heart attack and stroke over both 10 years and 30 years.
This matters because many younger adults may have a low 10-year risk but a much higher lifetime or 30-year risk. For example, a 42-year-old may not have a high chance of a heart attack in the next few years, but their long-term risk may be meaningful if LDL cholesterol, blood pressure, diabetes risk, or family history are concerning.
The 2026 guideline classifies 10-year PREVENT-ASCVD risk as:
- <3% — Low risk
- 3% to <5% — Borderline risk
- 5% to <10% — Intermediate risk
- 10% or higher — High risk
These categories help guide whether lifestyle alone is reasonable or whether medication should be added.
7. Is all calcified plaque the same?
No. This is an important point.
Plaque can behave differently depending on its structure. Some plaque is more stable, while other plaque is more likely to rupture and cause a heart attack.
Stable calcified plaque
A stable plaque is usually more hardened and scar-like. It often has larger, denser calcium deposits, sometimes called macrocalcifications.
Stable plaque is still a sign of coronary artery disease, but it may be less likely to suddenly rupture. Think of it as a hardened scar in the artery wall. It tells us there has been damage, but it may be more structurally reinforced.
Unstable or vulnerable plaque
An unstable plaque is more concerning because it is more likely to rupture. These plaques often contain a soft, cholesterol-rich center, inflammation, and a thin outer covering. They may also have tiny scattered calcium spots, sometimes called microcalcifications or "spotty calcium."
These small calcium spots can create stress points in the plaque. If the plaque ruptures, the body may form a blood clot at that site. If the clot blocks blood flow to the heart muscle, it can cause a heart attack.
The important patient message is this: calcium tells us plaque is present, but a standard CAC score does not show every detail about plaque behavior.
8. Can my calcium score tell whether my plaque is stable or unstable?
Not perfectly.
This is one of the most common misunderstandings about the test.
A standard CAC score tells us the total amount of calcified plaque in the coronary arteries. It does not show all soft plaque, inflammation, thin fibrous caps, or the exact rupture risk of each plaque.
So the CAC score is best understood as a risk marker. It tells us whether coronary plaque is present and how much calcified plaque there is. It does not point to one exact plaque and say, "This one will cause a heart attack."
That is why CAC scoring is mainly used for prevention planning, not for deciding who needs a stent.
9. Why can statins raise the calcium score but still lower risk?
This surprises many patients.
Statins lower LDL cholesterol and reduce the risk of heart attack and stroke. Over time, statins may also change plaque composition. They can reduce softer, cholesterol-rich plaque and make plaque more calcified and dense.
Because the Agatston calcium score gives extra weight to denser calcium, the number may rise even while the plaque is becoming more stable. The American College of Cardiology has described this as part of the "plaque density paradox": statins may increase calcium density, which can raise the CAC score, while still lowering cardiovascular risk.
In other words, a rising calcium score after starting a statin does not always mean the treatment is failing.
The more important questions are:
- Did your LDL cholesterol come down enough?
- Is your blood pressure controlled?
- Are blood sugar and diabetes risk addressed?
- Are you exercising and avoiding smoking?
- Are you having symptoms?
- Was repeating the CAC scan even necessary?
For many patients with a known positive calcium score, the goal is not to keep chasing repeat scans. The goal is to treat risk factors aggressively and prevent heart attack or stroke.
10. If my calcium score is zero, am I safe?
A CAC score of 0 is generally good news. It means there is no visible calcified plaque on the scan.
For many patients, CAC 0 is associated with a lower short-term risk of heart attack. In selected patients, a score of 0 may support delaying statin therapy, especially if there is no diabetes, no smoking, and no strong family history of early heart disease.
But CAC 0 does not mean risk is zero. It does not rule out soft, non-calcified plaque. It also does not mean cholesterol, blood pressure, nutrition, sleep, exercise, and smoking no longer matter.
A score of 0 is reassuring. It is not a lifetime warranty.
11. If my calcium score is above zero, what should my LDL goal be?
This is one of the biggest updates from the 2026 ACC/AHA/Multisociety Dyslipidemia Guideline.
The guideline brings back LDL cholesterol goals and links them to overall risk and plaque burden. For people with subclinical atherosclerosis, including CAC, the LDL goals become more aggressive as the calcium score rises.
- CAC 1–99 and below 75th percentile — LDL-C goal <100 mg/dL
- CAC 100–299 or CAC ≥75th percentile — LDL-C goal <70 mg/dL
- CAC ≥1000 — LDL-C goal <55 mg/dL
This does not mean every patient needs the same medication. But it does mean that once plaque is seen, LDL cholesterol becomes a major treatment target.
For many patients, the first medication is a statin. If LDL cholesterol does not come down enough, other medications such as ezetimibe, bempedoic acid, or a PCSK9 inhibitor may be considered depending on the level of risk and the LDL response. The 2026 guideline notes that nonstatin therapies can be added when lifestyle and statins do not lower LDL-C enough.
12. If my calcium score is high, do I need a stent?
Usually, no.
A high calcium score means you have coronary plaque and a higher future risk of heart disease. It does not automatically mean you have a severe blockage that needs a stent.
Stents are usually used for certain patients with symptoms, abnormal stress testing, or acute heart problems. They are not placed simply because the calcium score is high.
If your CAC score is high, the most important next step is usually an aggressive prevention plan. This may include:
- Lowering LDL cholesterol
- Controlling blood pressure
- Treating diabetes or prediabetes
- Stopping smoking
- Exercising regularly
- Improving nutrition
- Managing weight when appropriate
- Addressing sleep and stress
- Considering additional cholesterol-lowering medications when needed
The calcium score is a warning light. It is not an automatic ticket to the cath lab.
13. Now that I have a CAC score, do I need a stress test?
Usually, not automatically.
A calcium score and a stress test answer different questions.
A CAC scan asks: "Is there calcified plaque in the heart arteries, and how much is there?"
A stress test asks: "Is blood flow to the heart muscle reduced during exercise or stress?"
If you feel well and do not have symptoms, a stress test is often not needed just because the calcium score is abnormal. Choosing Wisely Canada recommends against stress cardiac imaging or advanced noninvasive imaging in patients without cardiac symptoms unless high-risk markers are present.
When you may not need a stress test
You may not need a stress test if you have:
- No chest pain or chest pressure
- No shortness of breath with activity
- No unexplained decline in exercise capacity
- No fainting or concerning palpitations
- No abnormal ECG concerns
- No symptoms that occur with exertion and improve with rest
For example, if your CAC score is 150 and you feel well, the next step is usually preventive treatment, not an automatic stress test.
When a stress test may be helpful
A stress test may be appropriate if you have symptoms such as:
- Chest pressure, tightness, burning, or heaviness
- Shortness of breath with exertion
- New fatigue or reduced exercise tolerance
- Jaw, arm, back, or upper abdominal discomfort with activity
- Symptoms that improve with rest
- Abnormal ECG findings
- Very high CAC score plus clinical concern based on your full risk profile
If you have symptoms, your doctor may recommend a stress test, coronary CT angiogram, or another type of heart evaluation depending on your situation.
The simple rule is this: a calcium score helps guide prevention. Symptoms help decide whether we need to look for a blood-flow problem.
14. How does CAC affect statin decisions?
This is one of the most useful roles of CAC scoring.
A statin is a medication that lowers LDL cholesterol and reduces the risk of heart attack and stroke. But some patients are unsure whether they need one. CAC can help make that decision more personal.
The 2026 guideline supports CAC testing when a person's risk is borderline or intermediate and the decision about medication is uncertain. Having any CAC supports at least an LDL-C goal of <100 mg/dL, with lower LDL-C goals as the score rises.
A practical way to think about it:
- CAC 0: May support delaying medication in selected low-risk patients.
- CAC 1–99: Plaque is present; LDL-C goal is generally <100 mg/dL.
- CAC 100–299: More plaque is present; LDL-C goal is generally <70 mg/dL.
- CAC 300–999: High plaque burden; treatment should usually be more aggressive.
- CAC ≥1000: Very high plaque burden; LDL-C goal is generally <55 mg/dL.
The goal is not to treat the number alone. The goal is to reduce future heart attack and stroke risk.
15. What about aspirin?
Aspirin is more complicated.
Years ago, aspirin was commonly used for prevention. Today, doctors are more careful because aspirin can increase the risk of bleeding.
A high CAC score may sometimes support a discussion about aspirin, but aspirin should not be started automatically. The decision depends on your age, bleeding risk, stomach ulcer history, kidney function, other medications, and overall cardiovascular risk.
This is a conversation to have with your clinician.
16. Should I get Lp(a) or ApoB checked?
Often, yes — especially if your risk is not clear.
The 2026 ACC/AHA/Multisociety Dyslipidemia Guideline recommends that Lp(a) be measured at least once in adulthood. Lp(a), pronounced "L-P-little-a," is a mostly inherited cholesterol-related particle that can increase heart disease risk. Lifestyle changes have little effect on Lp(a), so it usually does not need to be checked over and over.
ApoB is another blood test that can help estimate the number of cholesterol-carrying particles in the blood. The guideline notes that ApoB can be useful in selected people, including those with diabetes, high triglycerides, cardiovascular-kidney-metabolic risk, or known cardiovascular disease, especially when LDL-C alone may not tell the full story.
For patients with a positive CAC score, these tests can sometimes help decide how aggressive LDL-lowering therapy should be.
17. Is the calcium score test safe?
A CAC scan is quick and noninvasive. It usually does not require IV contrast.
The radiation dose is relatively low compared with many other CT scans, but it is still radiation. RadiologyInfo lists cardiac CT for calcium scoring at about 1.7 mSv, which is roughly comparable to about 6 months of natural background radiation.
Because there is some radiation exposure, the test should be used when the result can change management.
18. Are there downsides to CAC scoring?
Yes. CAC scoring is helpful, but it is not perfect.
Possible downsides include:
- Radiation exposure
- Incidental findings, such as lung nodules
- Anxiety from seeing a high score
- False reassurance from a score of 0
- Cost, since insurance coverage varies
- Unnecessary follow-up testing if the result is not interpreted carefully
- Limited information about soft plaque or whether a specific blockage is severe
This is why CAC scoring should be used as part of a prevention discussion, not as a stand-alone answer.
19. How often should CAC be repeated?
It depends.
If your CAC score is 0, repeating the test years later may be reasonable in selected patients, especially if risk factors change. If your CAC score is already clearly positive, repeating the test is often less useful. The plaque is already present. The main job is to treat the risk factors.
In many cases, it is better to follow:
- LDL cholesterol response
- Blood pressure
- Blood sugar
- Weight and waist circumference
- Exercise habits
- Smoking status
- Symptoms
- Medication adherence
A repeat scan should answer a specific clinical question. Otherwise, it may just create another number to worry about.
20. What should I do after getting my CAC score?
Review the result with your clinician in the context of your full risk picture.
Important factors include:
- Age
- Sex
- Blood pressure
- LDL cholesterol
- HDL cholesterol
- Triglycerides
- Diabetes or prediabetes
- Smoking history
- Family history
- Kidney disease
- Inflammatory disease
- Pregnancy-related risk factors
- Lp(a)
- ApoB when appropriate
- Symptoms
Then make a prevention plan that fits your risk.
That plan may include lifestyle changes, cholesterol-lowering medication, blood pressure treatment, diabetes prevention or treatment, smoking cessation, and sometimes additional testing if symptoms are present.
21. What is the bottom line?
A coronary calcium score is one of the most useful tools in preventive cardiology when used for the right patient.
It can show whether silent coronary plaque is already present. It can help personalize decisions about statins and other prevention strategies. It can also motivate action before symptoms develop.
A score of 0 can be reassuring in the right setting. A score above 0 means plaque is present and LDL cholesterol goals should be discussed. A score above 100 is a strong signal to take prevention seriously. A very high score means the prevention plan should be more aggressive.
But a calcium score is not a crystal ball. It does not show every type of plaque. It does not automatically mean you need a stress test or a stent. And it should always be interpreted in the context of your symptoms, risk factors, and overall health.
The goal is simple: find risk early, treat it wisely, and prevent the heart attack that never needed to happen.
Comments
No comments yet. Be the first to share your thoughts.
Sign in to join the conversation.
Sign In